



版权说明:本文档由用户提供并上传,收益归属内容提供方,若内容存在侵权,请进行举报或认领
文档简介
1、The Role of Drugs in Prevention of Sudden Cardiac Death Weimin Li Professor of Medicine Cardiovascular Department, the First Clinical Hospital, Harbin Medical University,Harbin Presentation Overview Sudden Cardiac Death Epidemiology, etiology, pathophysiology Overview of ICD therapy to prevent SCD R
2、oles of Drugs in SCD Prevention Summary and conclusionsEpidemiology of SCDn Accounts for 63% of all cardiac related deaths in the US. n One of the most common causes of death in developed n countries: MMWR. Vol 51(6) Feb. 15, 2019. Myerberg RJ, Catellanos A. Cardiac Arrest and Sudden Cardiac Death.
3、In: Braunwald E, ed. Heart Disease: A Textbook of Cardiovascular Medicine. 5th Ed. New York: WB Saunders. 2019: 742-779. Zheng Z. Circulation. 2019;104:2158-2163. Vreede-Swagemakers JJ et al. J Am Coll Cardiol 2019; 30: 1500-1505.WorldwideUS300,000350,0003,000,000W.Europe400,000Magnitude of SCD in C
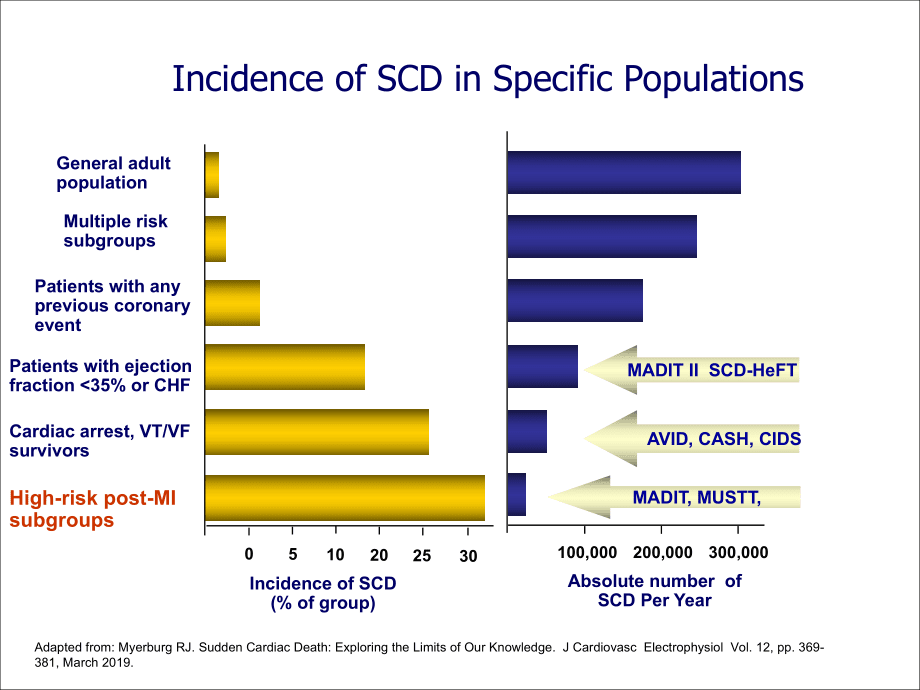
4、hina0.1%0.04%0.2%ChinaUS544,000300,000350,000ChinaUSIncidence RateAbsolute Number0.04%0.1%0.2%Incidence of SCD in Specific Populations Adapted from: Myerburg RJ. Sudden Cardiac Death: Exploring the Limits of Our Knowledge. J Cardiovasc Electrophysiol Vol. 12, pp. 369-381, March 2019. 300,000200,0001
5、00,000Absolute number of SCD Per Year Multiple risk subgroupsPatients with any previous coronary eventPatients with ejectionfraction 35% or CHFCardiac arrest, VT/VF survivorsHigh-risk post-MI subgroupsGeneral adult population3025201050Incidence of SCD(% of group) MADIT II SCD-HeFT AVID, CASH, CIDS M
6、ADIT, MUSTT, nSudden death was the first manifestation of coronary heart disease in 50% of men and 63% of women. nCHD accounts for at least 80% of sudden cardiac deaths in Western cultures.80%Coronary Heart Disease15% Cardiomyopathy5% Other Disease Cause of SCDAmerican Heart Association. Heart Disea
7、se and Stroke Statistics2019 Update. Dallas, Tex.: American Heart Association; 2019. Adapted from Heikki et al. N Engl J Med, Vol. 345, No. 20, 2019.Myerberg RJ. Heart Disease, A Textbook of Cardiovascular Medicine. 6th ed. P. 895.Arrhythmic Cause of SCDAlbert CM. Circulation. 2019;107:2096-2101.12%
8、Other Cardiac Cause88%Arrhythmic CauseBradycardia16.5%VF62.4%Primary VT8.3%Torsades de Pointes12.7%Bays de Luna A. Am Heart J. 1989;117:151-159.Application of ICD in China200544,000“Even the wealthiest nations cannot afford to pay to use every medical advance in any patient who might benefit.Thomas
9、Bigger, Lancet, 2019Roles of Drugs in SCD PreventionRoles of Drugs in SCD PreventionValue of Antiarrhythmic Drugs Class I antiarrhythmics Beta Blockers Amiodarone SotalolValue of Non-antiarrhythmic Drugs Electrolytes ACE inhibitors, ARBs and aldosterone blockers Antithrombotic and antiplatelet agent
10、s Statins n-3 Fatty acidsSCD Prevention by Antiarrhythmic DrugsAll-cause mortalityDays after randomization050100 150 200 250 300 350 400 450 500859095100Survival(%)Placebo (n=725)Encainide or flecainide (n=730):406CAST Investigators. N Engl J Med 1989;32112.P=0.000380 Roles of Class I antiarrhythmic
11、s in SCD PreventionCAST: Cardiac Arrhythmia Suppression TrialCAST II: Cardiac Arrhythmia Suppression Trial II As with the antiarrhythmic agents used in CAST-I, the use of moricizine in CAST-II to suppress asymptomatic or mildly symptomatic ventricular premature depolarizations to try to reduce morta
12、lity after myocardial infarction is not only ineffective but also harmful.Roles of Beta Blockers in SCD PreventionStudyBHATNorwegianCOPERNICUSCIBIS-IICAPRICORNMERIT-HFPublished1981Follow upTarget Dosage(mg/day)Patientsmild/moderate HFPost-MI LVDPost-MI LVDPost-MI LVDmoderate/severe HFsevere HFDrugPr
13、opranoloTimololmetoprololcarvedilolbisoprololcarvedilol 200 qd 25 bid 10 bid 180240 25 bid 10 qd25m17m15m2.4y1.3y10.4m19822000201920192019 Norwegian Multicentre Study Group. N Engl J Med. 1981;304:801-807.36333027242118151296300.000.050.100.150.200.25TimololPlaceboMonthCumulative Mortality Raten=945
14、n=939P0.0005Overview of Norwegian Timolol Trialand BHAT(Beta-Blocker Heart Attack) Trial (Post-MI LVD patients) 39% Reduced mortality Placebo n=1921061824303612024681012N=383737063647395921631310406Cumulative Mortality (%)Months of Follow-upPropranolol n=1916P0.00526% Decreased mortalityBeta-Blocker
15、 Heart Attack Trial Research Group. JAMA. 1982;247:1707-1714.BHATNorwegianAverage incidence of SCD in long term trials comparing blockers with placebo after MINuttall SL, Toescu V, Kendall MJ. BMJ. 2000;320:581.Average incidence of sudden death in long term trials comparing - blockers with placebo a
16、fter myocardial infarction Placebo treatment Blocker treatment Total No of patientsTotal No of deathsNo (%) of sudden deathsTotal No ofpatientsTotal No of deathsNo (%) of sudden deathsNorwegian timolol trial 93915295 (63) 945 9847 (48)Blocker heart attack trial192118889 (47)191613864 (46)PlaceboCarv
17、edilolHazard Ratio(95% CI)Cardiovascular Death1040.75(0.58-0.96)Sudden Death69510.74(0.51-1.06)Death Due to Pump Failure30180.60(0.33-1.07) CAPRICORN: Carvedilol Post-Infarct Survival Control in LV Dysfunction - TRIAL RESULTS - Dargie HJ et al. Eur J Heart Fail. 2000;2:325-332. CIBIS II: Cardiac Ins
18、ufficiency Bisoprolol Study II - RESULTS -PPrimary endpoint All-cause mortality Secondary endpoints All-cause hospital admission All cardiovascular deaths Combined endpoint Exploratory analyses Sudden death Hospital admission for worsening heart failure17 39 12 35 6 1812 33 9 29 4 120.66 (0.54 0.81)
19、 0.80 (0.71 0.91) 0.71 (0.56-0.90)0.79 (0.69 0.90) 0.56 (0.39 -0.80) 0.64 (0.53 0.79)0.0001 0.0006 0.0049 0.0004 0.0011 0.0001Primary and secondary outcomesPlacebo(n=1320)(%)(n=1327)(%)Hazard ratio(95% CI)CIBIS-II Investigators and Committees. Lancet 2019; 353MERIT-HF: Metoprolol CR/XL Randomized In
20、tervention Trial in congestive Heart Failure - RESULTS -MERIT-HF Study Group. Lancet 2019;353:20197.00.51.01.5Relative risk for mortalityRelative risk (95% CI)MortalityMetoprolol CR/XL betterRiskreduction(%)Total mortalityCardiovascular mortalitySudden deathDeath from worseningheart failure343841490
21、.00620.000030.00020.0023PCOPERNICUS: Carvedilol Prospective Randomized Cumulative Survival trial- SUMMARY - In patients with severe chronic heart failure, carvedilol in addition to standard therapy reduced: All-cause mortality Combined endpoint of all-cause mortality and hospitalization for any reas
22、onPacker M, Coats AJ, Fowler MB et al. N Engl J Med 2019;344:16518.Roles of Beta Blockers in SCD PreventionStudyBHATNorwegianCOPERNICUSCIBIS-IICAPRICORNMERIT-HFSCD Risk Reduction (p-value)DrugPropranoloTimololmetoprololcarvedilolbisoprololcarvedilolTotal Death Risk Reduction (p-value)34% (0.00009)23
23、% ( 0.031) 26%(0.005)39%(0.0005)35% ( 0.001)34% ( 0.0001)Not reportedNot reported26% ( 0.099) 41% ( 0.0002)44% ( 0.001)Not reported Roles of Amiodarone in SCD PreventionConnolly SJ. Meta-analysis of antiarrhythmic drug trials. Am J Cardiol 2019;84:90R3R. A meta-analysis of effects of amiodarone on S
24、CD Meta-analysis of effects of amiodarone on SCD-RESULTS- Cumulative risk of total mortality and arrhythmic/sudden death from a meta-analysisof 13 trials of amiodaroneAmiodaroneControlTotal mortalityArrhythmic/sudden death29% reduction inarrhythmic deathP=0.0003Meta-analysis of the ICD secondary pre
25、vention trialsConnolly SJ. et al.Meta-analysis of the implantable cardioverter defibrillator secondary prevention trialsEuropean Heart Journal. 2000; 20712078Meta-analysis of effects of amiodarone on SCD - RESULTS - Cumulative risk of fatal events or the amiodarone and treatment arms.Hazard ratio:0.
26、73P0.001Hazard ratio:0.49P35% and 35% The efficacy of the ICD over amiodarone appears to be dependent upon the degree of left ventricular dysfunction.MortalityFolow-up(m)Mortality by Intention-to-TreatSCD-HeFT-2019 HR 97.5% CI PAmiodarone vs placebo1.060.86, 1.30 0.529ICD therapy vs placebo0.770.62,
27、 0.96 0.007AmiodaroneICD therapyPlaceboBardy GH, Lee KL, Mark DB, et al. N Engl J Med, 2019, 352:225ICD + AADsPercent Arrhythmia-Free26%reduction inevent ratethe time to first event extended median 1.3 months to median 4.4 monthsSteinberg JS, Martins J, Sadanandan S, et al. Am Heart J. 2019;142:520-
28、529 ICD ICD + AADs Roles of Sotalol in SCD PreventionSWORD Survival Results1.000Time from randomisation (days)Z = -2.5, P = 0.006Proportion event-freePlacebod-sotalol60120180240300.99.98.97.96.95.94.93.92.91.90.89.88.87Patients at riskPlacebo15721170874551330d-sotalol15491150844544323Study stopped p
29、rematurely in Nov. 1994 due to increased mortality in patient population treated with d-sotalolWaldo AL. Lancet. 2019;348:7-12. Roles of Sotalol in SCD PreventionKuhlkamp V. Suppression of sustained ventricular tachyarrhythmias: a comparison of d,l-sotalol with no antiarrhythmic drug treatment. J Am
30、 Coll Cardiol.2019;33: 46-52.ICD/sotalolsotalolICDRoles of Antiarrhythmic Drugs in SCD PreventionValue of Antiarrhythmic Drugs Class I antiarrhythmics: not only ineffective but also harmful Beta Blockers: Effective in suppressing ventricular ectopic beats and arrhythmias; reduce incidence of SCD Ami
31、odarone: No definite survival benefit; some studies have shown reductionin SCD in patients with LV dysfunction, especially when given in conjunction with BB. but it has complex drug interactions and many adverse side effects. Sotalol: Suppresses ventricular arrhythmias; is more pro-arrhythmic than a
32、miodarone, no survival benefit clearly shown Conclusions: Antiarrhythmic drugs (except for BB) should not be used as primary therapy of the prevention of SCD. Both sotalol and amiodarone have been shown to reduce the frequency of ICD shock therapySCD Prevention by Non-antiarrhythmic DrugsRoles of an
33、giotensin converting enzyme inhibitors (ACEI) angiotensin receptor blockers(ARB) and aldosterone blocker in SCD PreventionRamiprilhigh-risk patients not known to have low ejection fraction or heart failure2000DrugPatientsStudyPublishedHOPESOLVDTEnalapril chronic heart failure1991EPHESUSEplerenonePos
34、t-MILV dysfunction2019RALESSpironolactonechronic heart failure2019CHARMCandesartanchronic heart failure2019SOLVDPEnalaprilchronic heart failure1991Meta-analysis of 15 randomized controlled trial - RESULTS -Domanski MJ, Exner DV, Borkowf CB, et al. JACC Vol. 33, No. 3,2019:598604ACEIACEIACEIACEIACEIM
35、eta-analysis of 15 randomized controlled trial - RESULTS -The overall OR for SCD in patients randomized to ACE inhibitor therapy was 0.80 (95% CI 0.70 to 0.92)ACEIs reduce the risk of SCD about 20% in post-MI patientsHOPE: Heart Outcomes Prevention Evaluation study- RESULTS -PPrimary outcome and dea
36、ths from any cause342The Hope Study Investigators. N Engl J Med 2000;:14553.Relative risk(95% CI)MI, stroke, or death fromcardiovascular causesDeath from cardiovascular causesMIStrokeDeath from noncardiovascular causesDeath from any causeRamipriln=4645(%)14.06.19.93.44.310.4Placebon=4652(%)17.88.112
37、.34.94.112.20.78 (0.700.86)0.74 (0.640.87)0.80 (0.700.90)0.68 (0.560.84)1.03 (0.851.26)0.84 (0.750.95)0.0010.0010.0010.0010.740.005Ramipril reduced the risk of SCD about 38% (0.02)N Engl J Med 1991;325:293-30216% Risk Reduction in All Cause Mortality p = 0.00360102030405006 12 18 24 30 36 42 48Month
38、sMortality%Placebo EnalaprilAll Cause Mortality and SCD SOLVD Treatment TrialSOLVD Prevention Trial10% Risk Reduction in SCD p = NS051015202506 12 18 24 30 36 42 48MonthsMortality (%)7% Risk Reduction in SCD p = NSCHARMCandesartan in Heart failure Assessment of Reduction in Mortality and morbidity -
39、 RESULTs -yrs3.50123010203052515CandesartanPlaceboNon CV deathp=0.6016% reductionp=0.005CV deathCV deaths and Non CV deaths (%)PlaceboCandesartanNumber at riskCandesartan2289210518942580Placebo2287202318111333548CHARM Candesartan in Heart failure Assessment of Reduction in SCD- RESULTs -The CHARM st
40、udy Investigators. Circulation. 2019;110:2618-26. Treatment of heart failure patients with candesartan resulted in a reduction in SCD (p=0.036)CHARM-AlternativeCHARM-AddedCHARM-PreservedCHARM-OverallCandecartan(n=1013) Placebo (n=1015)Candecartan(n=1276) Placebo (n=1272)Candecartan(n=1514) Placebo (
41、n=1508)Candecartan(n=3803) Placebo (n=3796)Hazard Ratioand 95% Ci8011115016869652993443.04.33.94.51.61.52.73.2SCD*Per 100 person-years 0.850.73-0.99P=0.036 Incidence rateRALES : the Randomized Aldactone Evaluation Study- RESULTs -PCardiac causesProgression of heart failureSudden death0.001 Cardiovas
42、cular deathSpironolactone group(n=822)3141891101522622782170.69 (0.580.82)0.64 (0.510.80)Placebo group(n=841)Raletive risk(95% CI)VARIABLEMyocardial infarction0.71 (0.540.95)0.020.001Pitt, N Engl J Med 2019; SCD Risk Reduction: 29% (p0.02) EPHESUS Treatment with eplerenone in the subgroup of patient
43、s with LVEF 30% resulted in relative risk reductions of 33% for SCD (P=0.008) Roles of angiotensin converting enzyme inhibitors (ACEI) angiotensin receptor blockers(ARB) and aldosterone blocker in SCD PreventionDrugTotal Death Risk Reduction (p-value)StudySCD Risk Reduction (p-value)HOPERamipril26%
44、(0.005)38% (0.02)SOLVDTEnalapril 16% (0.004)10% (NS)EPHESUSEplerenone8% (=0.02)58% (P=0.008) RALESSpironolactone30% (0.001)29% (0.02)CHARMCandesartan12% (p=0.018)Not reportedSOLVDPEnalapril8% (0.3)7% (NS)Roles of Antithrombotic Therapy in SCD PreventionData from SOLVD prevention and treatment trials
45、 Incidence and Crude Relative Risk of Sudden Coronary Death, Cardiovascular Death, and All-Cause Mortality According to Antithrombotic TherapyNeither 225 2.76 1.0 754 9.24 1.0 853 10.45 1.0Antiplatelet 149 1.82 0.66 470 5.75 0.63 534 6.48 0.63Anticoagulant 40 1.86 0.70 155 7.21 0.82 185 8.56 0.87Bot
46、h 10 2.24 0.81 34 7.61 0.83 37 8.28 0.8095% CI the 2-sided 95% confidence interval for the point estimate of the relative risk.Cardiovascular deaths include sudden cardiac death, death due to progressive pump failure, fatal myocardial infarction, and cerebrovascular deaths.The rate is expressed as e
47、vents per 100 patient-years of follow-up. RR relative risk.Sudden Coronary DeathCardiovascular Death All Cause MortalityNo. Rate RR No. Rate RR No. Rate RR Dries DL, et al. Am J Cardiol. 2019;79: 909-913Roles of Antithrombotic Therapy in SCD Prevention Antiplatelet and anticoagulant monotherapy each
48、 remained independently associated with a reduction in the risk of SCD: antiplatelet therapy with a 24% reduction. anticoagulant therapy with a 32% reduction. Thus, in patients with moderate to severe left ventricular systolic dysfunction resulting from coronary artery disease, antiplatelet and anticoagulant therapy are each associated with a reduction in the risk of SCD.Data from SOLVD prevention and treatment trials Roles of Statins in SCD PreventionStatins in the MADIT-II Study.Vyas AK, Hongsheng Guo, Moss AJ, et al.
温馨提示
- 1. 本站所有资源如无特殊说明,都需要本地电脑安装OFFICE2007和PDF阅读器。图纸软件为CAD,CAXA,PROE,UG,SolidWorks等.压缩文件请下载最新的WinRAR软件解压。
- 2. 本站的文档不包含任何第三方提供的附件图纸等,如果需要附件,请联系上传者。文件的所有权益归上传用户所有。
- 3. 本站RAR压缩包中若带图纸,网页内容里面会有图纸预览,若没有图纸预览就没有图纸。
- 4. 未经权益所有人同意不得将文件中的内容挪作商业或盈利用途。
- 5. 人人文库网仅提供信息存储空间,仅对用户上传内容的表现方式做保护处理,对用户上传分享的文档内容本身不做任何修改或编辑,并不能对任何下载内容负责。
- 6. 下载文件中如有侵权或不适当内容,请与我们联系,我们立即纠正。
- 7. 本站不保证下载资源的准确性、安全性和完整性, 同时也不承担用户因使用这些下载资源对自己和他人造成任何形式的伤害或损失。
最新文档
- 标准固定期限承包合同5篇
- 文化发展有限公司员工聘用协议书及员工保密合同6篇
- 2025年土建包清工合同5篇
- 农产品嫁接种苗技术服务合同5篇
- 民间担保贷款借资合同10篇
- 借款合同范本人民币委托贷款合同9篇
- 电力工程劳务合同范本
- 委托律师合同模板5篇
- 汾酒销售合同6篇
- 搜索算法的鲁棒性改进-全面剖析
- 国家职业技能标准 (2021年版) 婴幼儿发展引导员
- 幼儿园小班科学:《小鸡和小鸭》 PPT课件
- 伯努利方程-ppt课件
- 银行从业资格考试题库附参考答案(共791题精心整理)
- 年产20吨阿齐沙坦原料药生产车间的设计和实现材料学专业
- 沪宁城际接触网专业验收标准
- 电子公章模板
- 安徽省融资性担保公司代偿损失核销管理暂行办法
- 第3章轨道车辆牵引计算
- 基于JSP的校园网站的设计与实现论文
- 足球比赛登记表
评论
0/150
提交评论