



版权说明:本文档由用户提供并上传,收益归属内容提供方,若内容存在侵权,请进行举报或认领
文档简介
1、最新高血压指南的几个问题最新高血压指南的几个问题刘力生刘力生内容提要 关于血压水平的定义和分类关于血压水平的定义和分类 关于危险度分层关于危险度分层 关于卫生经济学关于卫生经济学 关于用药问题关于用药问题高血压患者危险分层高血压患者危险分层-WHO/ISH 1999血压血压( (mmHg)mmHg)其他危险因素和病史其他危险因素和病史1 1级级SBP 140SBP 140159159或或DBP90-99DBP90-992 2级级SBP 160-179 SBP 160-179 或或DBP 100-109DBP 100-1093 3级级SBP SBP 180 180 或或DBP DBP 11011
2、0I I 无其他危险因素无其他危险因素II 1-2II 1-2个危险因素个危险因素III III 3 3个危险因素或个危险因素或 器官损害或糖尿病器官损害或糖尿病IV IV 并存临床情况并存临床情况低危低危中危中危高危高危很高危很高危中危中危中危中危高危高危很高危很高危高危高危很高危很高危很高危很高危很高危很高危注:注:1999年中国高血压防治指南年中国高血压防治指南的危险分层参考的是的危险分层参考的是 1999年年WHO/ISH指南指南影响高血压患者预后的因素影响高血压患者预后的因素心血管危险因素心血管危险因素靶器官损害靶器官损害糖尿病糖尿病关联临床状况关联临床状况 血压水平血压水平 男性男
3、性55岁岁 女性女性65岁岁 吸烟吸烟 血脂紊乱血脂紊乱(TC6.5mmol/L, LDL-C4.0 mmol/L, HDL-C男男1.0,女,女1.2mmol/L) 早发心血管疾早发心血管疾病家族史病家族史(男男55, 女女102, 女女88cm) CRP 1 mg/dl 左心室肥厚左心室肥厚(心电图:(心电图:Sokolow-lyons38mm; Cornell2440mm*ms; 超声超声心动图:心动图:LVMI 男男 125,女女 110g/m2) 超声证实动脉壁增超声证实动脉壁增厚厚(颈动脉(颈动脉IMT 0.9mm)或粥样硬化斑块或粥样硬化斑块 血清肌酐轻微升高血清肌酐轻微升高(男
4、(男115-133,女,女107-124 mol/L) 微白蛋白尿症微白蛋白尿症(30-300mg/24H; 白蛋白白蛋白/肌酐比肌酐比值男值男 22,女,女 31) 空腹血浆葡空腹血浆葡萄糖萄糖7.0mmol/L 餐后血浆葡餐后血浆葡萄糖萄糖11.0mmol/L 脑血管疾病:脑血管疾病:缺缺血性脑卒中;脑出血;血性脑卒中;脑出血;一过性脑缺血发作一过性脑缺血发作 心血管疾病:心血管疾病:心心肌梗死;心绞痛;冠肌梗死;心绞痛;冠脉血运重建;心力衰脉血运重建;心力衰竭竭 肾脏病变:肾脏病变:糖尿糖尿病性肾脏病变;肾损病性肾脏病变;肾损害(肌酐升高男害(肌酐升高男133,女女124 mol/L);
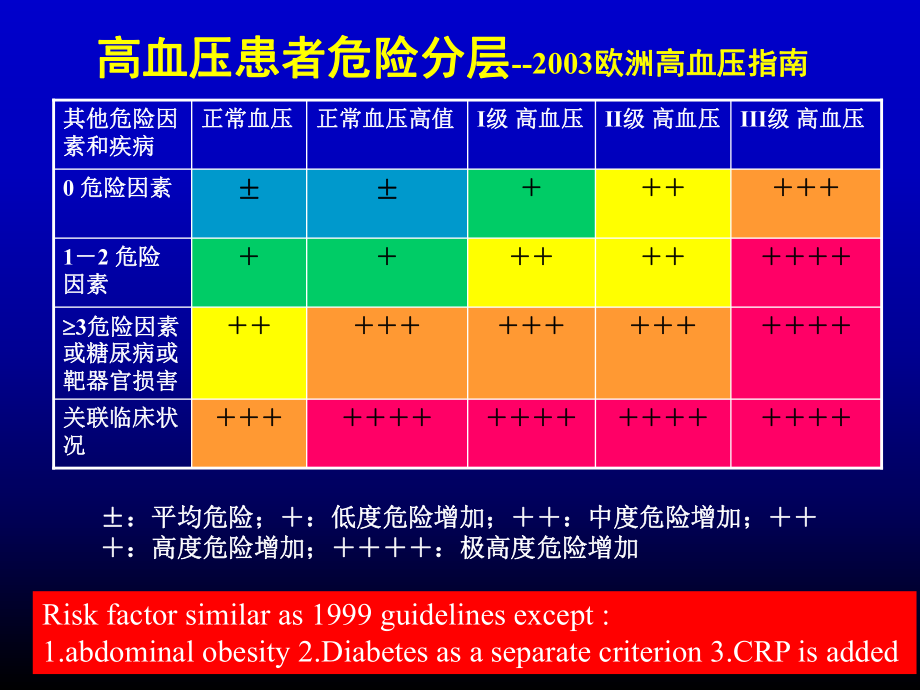
5、蛋);蛋白尿(白尿(300mg/24H) 周围血管疾病周围血管疾病 高度眼底病变:高度眼底病变:出血;或渗出,乳头出血;或渗出,乳头水肿水肿高血压患者危险分层高血压患者危险分层-2003欧洲高血压指南欧洲高血压指南III级级 高血压高血压II级级 高血压高血压I级级 高血压高血压正常血压高值正常血压高值正常血压正常血压其他危险因其他危险因素和疾病素和疾病关联临床状关联临床状况况 3危险因素危险因素或糖尿病或或糖尿病或靶器官损害靶器官损害12 危险危险因素因素0 危险因素危险因素:平均危险;:低度危险增加;:中度危险增加;:平均危险;:低度危险增加;:中度危险增加;:高度危险增加;:极高度危险增
6、加:高度危险增加;:极高度危险增加Risk factor similar as 1999 guidelines except :1.abdominal obesity 2.Diabetes as a separate criterion 3.CRP is added 血压分类血压分类-JNC-VI(1997)-JNC-VI(1997)-类类 别别 收缩压(收缩压(mm Hg) ) 舒张压(舒张压(mm Hg) )-理想血压理想血压 120 80120 80正常血压正常血压 120 - 129 80 - 84120 - 129 80 - 84正常高值正常高值 130 - 139 85 - 891
7、30 - 139 85 - 891 1级高血压级高血压 140 140 159 90 159 90 99 99 亚组:临界高血压亚组:临界高血压 140 - 149 90 - 94140 - 149 90 - 942 2级高血压级高血压 160 - 179 100 -109160 - 179 100 -109 3 3级高血压级高血压 180180 110110 单纯收缩期高血压单纯收缩期高血压 140140 90 90亚组:临界收缩期高血压亚组:临界收缩期高血压 140 - 149 90140 - 149 90- 1. Distribution of NHANES I Epldemiologi
8、c Follow-up Study Participants with a High-Normal BP or Hypertension at Baseline According to BP Lovel and Risk Categorization640(9.0)107(1.5)257(3.6)276(3.9)Risk Group A1366(19.2)5084(71.7)Total483(6.5)1505(21.2)160/ 100609(8.5)2208(31.1)140-159/90-99300(4.2)1371(19.3)130-139/85-89Risk Group CRisk
9、Group BSBP/DBP, mmHgValues are n (%)2. Estimated Effect of a 12mmHg Reduction in SBP Over 10 years on the Number-Needed-to-Treat to Prevent a Cardiovascular Disease Event Among NHANES I Epidemiologic Follow-Up Study Participants According to Baseline BP Level and Category of Presumed Cardiovascular
10、RiskRisk Group CRisk Group BRisk Group A8167131016160/ 10091711192033140-159/90-99101913232541130-139/85-89Corrected*UncorrectedCorrected*UncorrectedCorrected*UncorrectedSBP/DBP, mmHgSee test or Table 1 for deflnition of risk groups.*Corrected for regression dilution bias using a reliability coeffic
11、ient or 0.53 to correct for Imprecision in the measurement of SBP,3. Estimated Effect of a 12mmHg Reduction in SBP Over 10 years on the Number-Needed-to-Treat to Prevent a Cardiovascular Disease Death Among NHANES I Epidemiologic Follow-Up Study Participants According to Baseline BP Level and Catego
12、ry of Presumed Cardiovascular RiskRisk Group CRisk Group BRisk Group A112012213449160/ 10018312744273394140-159/90-9921373660486701130-139/85-89Corrected*UncorrectedCorrected*UncorrectedCorrected*UncorrectedSBP/DBP, mmHgSee test or Table 1 for deflnition of risk groups.*Corrected for regression dilu
13、tion bias using a reliability coefficient or 0.53 to correct for Imprecision in the measurement of SBP,4. Estlmated Effect of a 12mmHg Reduction in SBP Over 10 years on the Number-Needed-to-Treat to Prevent An AI-Cause Death Among NHANES I Epidemiologic Follow-Up Study Participants According to Base
14、line BP Level and Category of Presumed Cardiovascular RiskRisk Group CRisk Group BRisk Group A9169172337160/ 100122216276097140-159/90-991425193381130130-139/85-89Corrected*UncorrectedCorrected*UncorrectedCorrected*UncorrectedSBP/DBP, mmHgSee test or Table 1 for definition of risk groups.*Corrected
15、for regression dilution bias using a reliability coefficient or 0.53 to correct for Imprecision in the measurement of SBP不同危险程度高血压患者的血压水平不同危险程度高血压患者的血压水平(mmHg, x s) 男男 女女危险度危险度 SBP DBP SBP DBP低危低危 141.3(12.0)88.7(7.9)141.7(10.8)88.4(10.1)中危中危 144.7(15.6)89.3(9.7)144.1(26.7)86.4(10.6)高危高危 144.0(17.7)
16、88.8(11.5)139.6(18.6)85.6(14.5)极高危极高危 148.4(21.5)*88.8(12.8)145.9(22.6)*87.6(34.2) * P0.05心血管危险度分层的重要性心血管危险度分层的重要性(一)(一)高血压常常伴随其它危险因素高血压常常伴随其它危险因素降压治疗的目的是减少心血管发病与死亡降压治疗的目的是减少心血管发病与死亡(CVD Risk),而不仅是降低血压(而不仅是降低血压(RFs),所以,所以对心血管危险的估算是不可或缺的对心血管危险的估算是不可或缺的血压升高是血压升高是CVD RR 的重要指标,故以往只看的重要指标,故以往只看血压水平决定治疗策略
17、。此法对中重度高血压行血压水平决定治疗策略。此法对中重度高血压行之有效,对轻度高血压则否之有效,对轻度高血压则否 心血管危险度分层的重要性(二)心血管危险度分层的重要性(二) NHANES-I根据根据 JNC VI,对,对7,090NHEFS队列队列20年随访说明临床决策不仅依靠平均血压水平,并年随访说明临床决策不仅依靠平均血压水平,并需考虑其他危险因素需考虑其他危险因素 1999年医院门诊人群高血压抽样调查报告表明年医院门诊人群高血压抽样调查报告表明,对对门诊高血压患者的危险度评估中门诊高血压患者的危险度评估中,如果只注意血压如果只注意血压水平水平,是很不够的是很不够的,会明显低估危险度会明
18、显低估危险度,必须全面评估必须全面评估其他危险因素其他危险因素,才能作出正确的判断才能作出正确的判断.Problems With a Strategy Based on Absolute Cardiovascular RiskF. Olaf Simpson/Journal of Hypertension 1996, Vol 14 No 6The proposed New Zealand guidelines: the 10-year absolute CVD risk strategy Consequences of the 10-year absolute-risk strategy Pos
19、sible age-related modifications of the 10-year absolute-risk strategyProblems raised by inclusion of other risk factors in the calculationsProblems in calculation of the expected gains from antihypertensive therapyProblems in calculations of CVD risk from raised blood pressureArticle 1Cardiovascular
20、 risk evaluation:an inexact science (1) Failure to consider the full risk of the metabolic syndrome in current guidelines Failure to appreciate the total benefit of antihypertensive therapy Excessive weighting of advanced age in the assessment of cardiovascular risk How accurate is current risk asse
21、ssment for uncomplicated mild hypertension?Although the absolute risk assessment methods may lack sufficient sensitivity, they still represent an improvement over that only the level of blood pressure and prior cardiovascular disease were relevant to therapeutic-decision making. To date, cardiovascu
22、lar risk evaluation is an inexact science.Cardiovascular risk evaluation: an inexact science (2)Enhancing risk stratification in hypertensive subjects: How far should we go in routine screening for target organ damage? First, it appears timely to include the search for microalbuminuria as a routine
23、component of the work-up of all hypertensive patients worldwide; Second, it seems reasonable to recommend that the search for target organ damage should extend to cardiac and carotid ultrasound for high risk and very high risk hypertensive subjects.Pharmacological Treatment of HypertensionJ D Swales / The Lancet Vol 344. Aug. 6, 1994Benefits of treatmentTreatment of severe hypertension Mild to moderate hypertension Defining the high-risk patient Value of repeated measurementsSystolic hypertensionTarget blood pressureSelection of therapy
温馨提示
- 1. 本站所有资源如无特殊说明,都需要本地电脑安装OFFICE2007和PDF阅读器。图纸软件为CAD,CAXA,PROE,UG,SolidWorks等.压缩文件请下载最新的WinRAR软件解压。
- 2. 本站的文档不包含任何第三方提供的附件图纸等,如果需要附件,请联系上传者。文件的所有权益归上传用户所有。
- 3. 本站RAR压缩包中若带图纸,网页内容里面会有图纸预览,若没有图纸预览就没有图纸。
- 4. 未经权益所有人同意不得将文件中的内容挪作商业或盈利用途。
- 5. 人人文库网仅提供信息存储空间,仅对用户上传内容的表现方式做保护处理,对用户上传分享的文档内容本身不做任何修改或编辑,并不能对任何下载内容负责。
- 6. 下载文件中如有侵权或不适当内容,请与我们联系,我们立即纠正。
- 7. 本站不保证下载资源的准确性、安全性和完整性, 同时也不承担用户因使用这些下载资源对自己和他人造成任何形式的伤害或损失。
最新文档
- 医院住院综合楼建设项目发展前景与实施方案分析
- 公民道德建设行动计划
- 地块平整项目实施方案优化升级
- 标准化厂房建设项目设计方案解析
- 提升品牌美誉度的有效途径计划
- 技术研发路线图计划
- 创造长期价值的工作计划设计
- 班主任的时间管理与工作效率计划
- 人事档案信息化管理计划
- 个人信用评分与贷款利率的关系试题及答案
- 建筑工程安全知识课件
- 钢材三方采购合同范本
- 贸易安全培训管理制度
- 全民营养周知识讲座课件
- 2025年郑州电力职业技术学院单招综合素质考试题库及答案1套
- 门牌安装施工方案
- GB/T 24477-2025适用于残障人员的电梯附加要求
- 螺栓紧固标准规范
- 风力发电项目合作框架协议
- 社区时政考试试题及答案
- 2025-2030中国PH传感器行业市场发展趋势与前景展望战略研究报告
评论
0/150
提交评论