



版权说明:本文档由用户提供并上传,收益归属内容提供方,若内容存在侵权,请进行举报或认领
文档简介
1、 副主任医师休 克Shock Syndrome1休克(Shock)的定义休克是指任何原因引起有效循环血量减少,导致组织和器官氧合血液灌流不足, 从而发生的代谢障碍和功能细胞受损的病理过程Shock is a condition in which the cardiovascular system fails to perfuse tissues adequately. Inadequate tissue perfusion can result in:generalized cellular hypoxia (starvation)widespread impairment of cellul
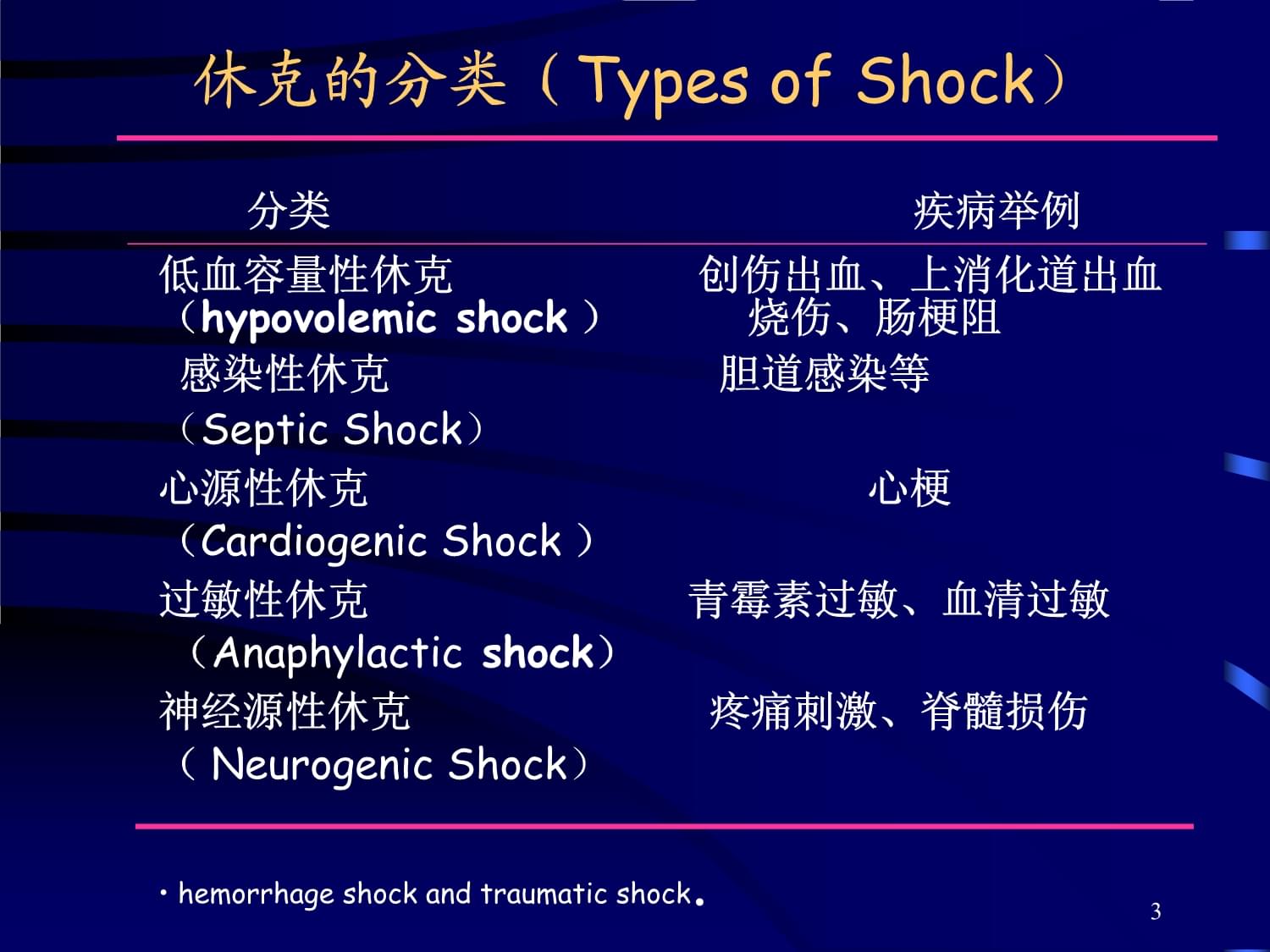
2、ar metabolismtissue damage organ failuredeath维持有效循环血量的必要因素: 充足的血容量 Sufficient blood volume有效的心排出量 Effective cardiac pump 良好的周围血管张力 Upstanding peripheral angiotasisEffective circulating blood volume2休克的分类(Types of Shock) 分类 疾病举例低血容量性休克 创伤出血、上消化道出血 (hypovolemic shock ) 烧伤、肠梗阻 感染性休克 胆道感染等(Septic Shock)
3、心源性休克 心梗(Cardiogenic Shock )过敏性休克 青霉素过敏、血清过敏 (Anaphylactic shock) 神经源性休克 疼痛刺激、脊髓损伤( Neurogenic Shock) hemorrhage shock and traumatic shock.3PATHOPHYSIOLOGY OF SHOCK SYNDROME微循环改变 Microcirculation Change代谢变化 Metabolism Change内脏器官的继发性损害 Secondary damage on internal organs4Microcirculation ChangeDecomp
4、ensated phaseCompensated phaseIrreversible phaseDeath5Sympathetic nervous system activatesCardiac effects Increased force of contractions Increased heart rate Increased cardiac outputPeripheral effects Arteriolar constriction Pre-/post-capillary sphincter contraction Increased peripheral resistance
5、Shunting of blood to core organsDecreased renal blood flowRenin released from kidney arterioleRenin & Angiotensinogen combineConverts to Angiotensin IAngiotensin I converts to Angiotensin IIPeripheral vasoconstrictionIncreased aldosterone release (adrenal cortex)Peripheral capillaries contain minima
6、l bloodStagnationAerobic metabolism changes to anaerobicCompensatory Mechanisms6休克的病理生理过程-微循环的变化微循环收缩期(休克代偿期)的特点: 心跳中枢、血管舒缩中枢、交感神经兴奋心跳加快,心排出量增加,儿茶酚胺大量释放儿茶酚胺的作用: 促使外周和内脏小、微血管和毛细血管前括约肌强烈收缩,动静脉短路和直捷通道开放收缩期结果: 外周血管阻力增加和回心血量增加;低灌注、缺氧状态。7Continued anaerobic metabolismRelaxation of precapillary sphinctersC
7、ontinued contraction of postcapillary sphinctersPeripheral pooling of bloodDecreased blood flow to the tissues causes cellular hypoxiaDecreased coronary blood flowMyocardial ischemiaDecreased force of contractionDecreased blood pressureDecompensated Shock8休克的病理生理过程-微循环的变化微循环扩张期(休克抑制期)的特点: 组织灌流不足,乏氧代
8、谢,酸性物质增多,微动脉和毛细血管前括约肌扩张,但毛细血管后静脉仍收缩 肥大细胞释放组胺,缓激肽,毛细血管扩张范围增加扩张期结果: 毛细血管多灌少流,容积增加,血液浓缩,回心血大减,心排血量减少,血压下降,心脑灌注不足,休克加重。 9If Low Perfusion States persists:IRREVERSIBLE DEATH IMMINENT!10Decreased perfusion causes tissue damage/necrosisTissue necrosis triggers diffuse clottingDiffuse clotting consumes clot
9、ting factorsFibrinolysis beginsSevere, uncontrolled systemic hemorrhage occursDisseminated Intravascular Coagulation (DIC)11休克的病理生理过程-微循环的变化微循环衰竭期(DIC期)的特点: 毛细血管内形成微血栓,DIC,细胞缺氧,组织自溶,由于凝血因子消耗,纤维蛋白溶解系统激活,出现严重的出血倾向12休克的病理生理变化体液代谢的改变能量不足(Energy deficiency)乏氧代谢(Anonic metabolism)致乳酸(Lactic acid)和丙酮酸(Pyru
10、vic acid)积聚,造成酸中毒(Metabolic acidosis) 钠泵(Sodium-pump)和钙泵(Calcium pump)功能异常,致细胞肿胀 ,甚至死亡13休克的病理生理变化内脏器官的继发性损害多器官衰竭 (Multiple Organ Systems Failure, MOSF):几个脏器相继或同时受损:呼吸窘迫综合征, ( ARDS: Adult respiratory distress syndrome )肾衰 (Renal failure):肾皮质内肾小管上皮变性坏死3. 心:心肌受损,局灶性坏死4. 肝功能衰竭 (Hepatic failure):小叶中央坏死5.
11、 胃肠道:粘膜糜烂、出血6. 脑:脑水肿(cerebral edema) 、脑疝(cerebral hernia) 14Stages of ShockInitial stage - tissues are under perfused, decreased CO, increased anaerobic metabolism, lactic acid is building Compensatory stage - Reversible. SNS activated by low CO, attempting to compensate for the decrease tissue perf
12、usion. Progressive stage - Failing compensatory mechanisms: profound vasoconstriction from the SNS ISCHEMIA Lactic acid production is high anaerobic metabolic acidosisIrreversible or refractory stage - Cellular necrosis and Multiple Organ Dysfunction Syndrome may occur DEATH IS IMMINENT!15Hypotensio
13、n 90 mmHg (may be normal level or increase due to compensatory mechanism) Mean arterial pressure (MAP) 60 mmHgTachycardia: weak and thready pulseTachypnea: blow off CO2 respiratory alkalosisDecreased urine outputGenerally Clinical Presentation16休克的临床表现休克代偿期: 丧失血容量20%1. 神志淡漠 (Disturbance of conscious
14、ness) 昏迷 (Coma) 2. 口唇 (Oral lip)、肢端 (Limb)发绀 (Cyanosis) ,出冷汗 (Cold sweat) 3. 脉细速 (Rapid rate and thread / weak pulse) ,血压下降 (Falling BP) ,脉压差 (Pulse pressure difference)明显缩小 4. 5. 尿量减少或无尿 (Anuria) 休克的临床表现18重度休克:血容量丧失40% 1. 昏迷 (Coma) 2. 全身皮肤粘膜紫绀 (Cyanosis),四肢冰冷 3. 脉搏摸不到,血压测不出 4. 无尿 (Anuria) 5. 器官功能衰竭
15、的表现休克的临床表现19休克的诊断Diagnosis of Shock早期诊断: 病史:失血、失液、创伤等 临床表现:兴奋或烦躁,出冷汗,心率快,脉压缩小,尿少抑制期诊断:依靠典型表现神志淡漠,反应迟钝,皮肤苍白或紫绀, 四肢湿冷,脉细速,呼吸浅快,收缩压下降至12kPa(90mmHg)以下,尿少或无尿20 神志状态 (Mental status) 肢体温度、色泽 (Limb temperature and color) 血压 (Blood pressure) 脉率 (Pulse) 尿量 (Urine output) 休克的监测一般监测General Monitor 21休克的监测特殊监测Sp
16、ecial Monitor 中心静脉压(Central Venous Pressure ,CVP): 血容量和心功能正常值:0.49-0.98 kPa (5-10cmH2O) CVP,血容量不足 CVP,心功能不全或过度收缩(1.47 kPa) 充血性心力衰竭 (Congestive Heart Failure) (1.96 kPa)22休克的监测特殊监测 Special Monitor 肺动脉楔压 (Pulmonary Capillary Wedge Pressure, PCWP) :可直接反映肺静脉、左心房和左心室的压力,了解肺循环阻力 正常值:0.8-2.0 kPa ,低于正常值,提示血
17、容量不足, 4.0 kPa,表示肺水肿心排出量和心脏指数:心排出量难以准确测定,临床应用少动脉血气分析 (Arterial Blood Gas Analysis ): 可了解呼吸功能和酸碱平衡的变化。 PaO2 80-100mmHg, PaCO2 36-44mmHg, PaCO260mmHg, PaO28 mmol/L, 死亡率100%。DIC的实验室检查确诊依据: Plat 80109/L; 纤维蛋白原3, 副凝实验(+);3P试验阳性;血涂片中破碎红细胞超过2%。24休克的治疗Treatment of Shock一般紧急措施 控制活动性大出血 休克体位: 头和躯干抬高20-30度, 下肢抬
18、高5-20度 吸氧,6-8L/min;保持呼吸道通畅 保持安静,避免搬动 保暖,可用休克服25休克的治疗 Treatment of Shock补充血容量 (Restore circulating volume and tissue perfusion) :是抗休克的根本措施 补充量:可根据CVP调节,应补充丧失量和已扩大的毛细血管床容量积极处理原发病 (Treat Reversible Causes) :在恢复有效血容量后积极手术处理外科原发病。在原发病不除,休克不能纠正时,应抗休克的同时,积极手术处理,以免丧失抢救时机26Shock treatment“A rude unhinging of
19、 the machinery of life”“A brief pause in the act of dying”27休克的治疗Treatment of Shock纠正酸碱平衡失调:主要是酸中毒 酸中毒的纠正有赖于休克的根本好转 补充血容量,改善组织灌流, 休克严重者,应给予碱性药物如碳酸氢钠心血管药物的应用 (Circulatory Support ) Vasoconstrictor :去甲肾上腺素;间羟胺;苯肾上腺素;苯苄胺;苄胺唑啉;多巴胺;异丙肾上腺素;西地兰等治疗DIC改善微循环皮质类固醇和其他药物的应用28In summary, Treatment of ShockIdentif
20、y the patient at high risk for shockControl or eliminate the causeImplement measures to enhance tissue perfusionCorrect acid base imbalanceTreat cardiac dysrhythmias29失血性休克的治疗(Treatment of Hemorrhagic Shock)补充血容量:根据情况输入晶体或/和胶体溶液 出血量少,无活动性出血者,输入晶体液 出血量大,有活动性出血者,先输晶体液,后输血 根据中心静脉压调整输液量和速度止血:在补充血容量的同时积极
21、止血 要处理好休克和止血手术间的辨证关系30中心静脉压和补液的关系CVP BP 原因 处理原则 低 低 血容量严重不足 充分补液 低 正常 血容量不足 适当补液 高 低 心功能不全 强心药,纠酸, 或血容量相对过多 舒血管 高 正常 容量血管过度收缩 舒张血管 正常 低 心功能不全 补液实验 或血容量不足 31损伤性休克的治疗 (Treatment of Traumatic Shock)补充血容量:应根据监测指标的变化来决定补液量纠正酸碱平衡失调:碱中毒酸中毒 适当应用碱性药物手术治疗:应根据病情判断是否需要手术以及手术时机的选择药物治疗:大量抗生素,复合维生素等32Hypovolemic S
22、hockManagement goal: Restore circulating volume and tissue perfusion:Control hemorrhageRestore circulating volumeOptimize oxygen deliveryVasoconstrictor if BP still low after volume loading33Aimed at improvement tissue hypoperfusion Insert Foley catheter to monitor the urine flow;Augment systolic bp
23、 to 100mmHg: 1. Place in reverse Trendelenburg position; 2. IV volume infusion (500-1000ml bolus), unless cardiogenic shock suspected (begin with normal saline, then whole blood, dextran, or packed RBCs, if anemic), continue volume replacement as needed to restore vascular volume;Add vasoactive drug
24、s after intrvascular volume is opmtimized; administer vasopressors if systemic vascular resistance is decreased. If severe metabolic acidosis is presented (pH7.15), administer NaHCO3;Identify and treat the underlying cause of shock.34感染性休克的特点Characteristics of Septic Shock内毒素性休克微循环变化的不同阶段常同时存在微循环变化和
25、内脏损害比较严重全身炎症反应综合征35感染性休克的类型Types of Septic Shock高排低阻型(高动力型): “Warm” shock hyperdynamic response, 原因:感染灶释放扩血管物质 特点:周围血管阻力降低,心排出量增加低排高阻型(低动力型) “Cold” shock hypodynamic response 原因:血容量减少+继发感染 活性因子:儿茶酚胺、5-羟色胺、组织胺、缓激肽 特点:周围血管阻力增加,心排出量降低36感染性休克的两种临床表现临床表现 冷休克(高阻力型) 暖休克(低阻力型)神志 躁动、淡漠或嗜睡 清醒皮肤色泽 苍白、紫绀或花斑样紫绀
26、淡红或潮红皮肤温度 湿冷或冷汗 温暖、干燥毛细血管充盈时间 延长 1-2秒脉搏 细速 慢、有力脉压(kPa) 4尿量(每小时) 30ml37Septic ShockTreatment:Prevention Find and kill the source of the infection Fluid resuscitationVasoconstrictorsInotropic drugsMaximize O2 delivery SupportNutritional Support38Treatment of Septic ShockAntibiotic treatment;Removal or
27、 drainage of a focal source of infection: Remove indwelling intravascular catheters and send tips for quantitative culture; replace Foley and other drainage catheters;Hemodynamic, respiratory, and metabolic support: . Maintain intravascular volume with IV fluids. Initiate treatment with 1-2L of norm
28、al saline administered over 1-2 h, keeping pulmonary capillary wedge pressure at 12-16 mmHg or central venous pressure at 8-12 cmH2O, urine output at30ml per hour, mean arterial blood pressure at 65mmHg. 39 Add inotropic and vasopressor therapy if needed. Maintain central venous oxygen saturation at
29、 70%. . Maintain oxygenation with ventilator support as indicated. Other treatments: Antiendotoxin, anti-inflammatory, and anticoagulant drugs are being studied in severe sepsis treatment.Anticoagulant recombinant activated protein C (aPC): constant infusion of 24ug/kg per hour for 96 h.Treatment of
30、 Septic Shock40感染性休克的治疗补充血容量:以平衡盐溶液为主,配合适量的血浆和全血;并根据CVP 调节输液量和速度控制感染:处理原发感染灶;应用抗菌药物;改善病人的一般状况;维持呼吸功能等纠正酸中毒:酸中毒发生早,严重,及早应用碱性药物心血管药物应用:西地兰;B-受体兴奋剂和a受体抑制剂联合应用减轻细胞损害:皮质类固醇,大剂量应用;SOD,抑肽酶,PGI2,试用中41THE END42Clinical examples-1An 82-year-old man was brought to the emergency room by his grandson, who report
31、ed that the man had been eating poorly for 2 days and had been difficult to arouse that morning. The patient had no specific complaints. On exam, the patient would open his eyes and mumble incoherently in response to pain. His temperature was 38.6, BP 75/40, HR 124 regular, respirations 26. His lung
32、s were clear. No murmurs or extra sounds were appreciated on cardiac exam. 43Clinical examples-1His skin was warm, with bounding peripheral pulses. His chest radiograph and EKG were normal. Laboratory data: white blood cell count 19500 (normal less than 10000). A bladder catheter was inserted (with
33、difficulty) and yielded cloudy urine, which was noted to contain many white cells and bacteria. Urine was sent for culture.44Clinical examples-2An 35-year-old woman presented to an emergency room complaining of a headache present since a myelogram which had been performed 4 days before. Her past med
34、ical history was unremarkable and her physical examination was normal. She was given an injection of meperidine for her pain. After the injection she began to complain of numbness and tingling in her fingertips, lightheadedness, shortness of breath and diffuse itching. 45Clinical examples-2Her pulse
35、 was noted to be 140 and blood pressure was palpable at 70/0 mmHg. Faint wheezes were noted throughout the lungs. Although she had initially denied drug allergies, she now remembered similar symptoms which had followed an injection of pain medicine” 2 years before.46Clinical examples-3An 67-year-old female arrived in the emergency room compl
温馨提示
- 1. 本站所有资源如无特殊说明,都需要本地电脑安装OFFICE2007和PDF阅读器。图纸软件为CAD,CAXA,PROE,UG,SolidWorks等.压缩文件请下载最新的WinRAR软件解压。
- 2. 本站的文档不包含任何第三方提供的附件图纸等,如果需要附件,请联系上传者。文件的所有权益归上传用户所有。
- 3. 本站RAR压缩包中若带图纸,网页内容里面会有图纸预览,若没有图纸预览就没有图纸。
- 4. 未经权益所有人同意不得将文件中的内容挪作商业或盈利用途。
- 5. 人人文库网仅提供信息存储空间,仅对用户上传内容的表现方式做保护处理,对用户上传分享的文档内容本身不做任何修改或编辑,并不能对任何下载内容负责。
- 6. 下载文件中如有侵权或不适当内容,请与我们联系,我们立即纠正。
- 7. 本站不保证下载资源的准确性、安全性和完整性, 同时也不承担用户因使用这些下载资源对自己和他人造成任何形式的伤害或损失。
最新文档
- 2026年智能吸顶式香氛机项目公司成立分析报告
- 2026年体征监测床垫项目公司成立分析报告
- 2026年卫星物联网开发项目可行性研究报告
- 2026年医疗影像设备AI辅助诊断系统项目公司成立分析报告
- 2026湖北事业单位联考咸宁市招聘132人备考题库附答案详解(能力提升)
- 2026贵州六盘水盘州市道路交通安全工作联席会议办公室社会招聘工作人员招聘7名备考题库含答案详解(基础题)
- 2026福建三明大田县总医院选聘城区分院工作人员的8人备考题库(含答案详解)
- 2026湖北事业单位联考荆门市钟祥市招聘141人备考题库附参考答案详解(培优)
- 2026年复合材料设计与仿真项目公司成立分析报告
- 2026湖南怀化市辰溪县供销合作联合社见习生招聘1人备考题库带答案详解(综合卷)
- 锰及化合物职业健康安全防护须知
- 2026年北京市房山区公安招聘辅警考试试题及答案
- 中建物资管理手册
- 嘉里大通物流公司员工行为规范指南
- 快易冷储罐知识培训课件
- 新能源材料与器件制备技术 课件 第5章 锂离子电池正极材料
- 消防监控证试题及答案
- 棋牌室转让合同协议书
- 吊车租赁合同范本
- 护理团体标准解读-成人氧气吸入疗法护理
- 高一英语暑假作业:Module 2(外研版必修1)
评论
0/150
提交评论